
An interesting read today from the blog of Dr Peter Fairbairn from EthOss about the common myths surrounding synthetic bone grafts.
This is the first in a series of three articles on this topic so stay tuned for parts 2 and 3 coming soon.
Happy reading!

I’ve been fortunate enough to lecture all over the world during my career and, whilst this is temporarily “on hold” due to all the problems caused by Covid-19, I am looking forward to speaking again in the future.
This lecturing has introduced me to fellow clinicians from all over the world and given me the opportunity to share expertise, techniques and experience with them. I am always amazed at how much I still have to learn, but something that I often find just as remarkable is the amount of “myths” and hearsay that have built up over the years surrounding synthetic graft materials.
These myths have penetrated the global conscious of our profession and I have heard them, in one form or the other, in every continent, country and city where I’ve lectured. I group them into 3 areas:
1) “Synthetic grafts lose their volume long-term, they aren’t stable and resorb too quickly”
2) “Without a collagen membrane you will get soft tissue ingress”
3) “Synthetic grafts are too technique sensitive, they don’t work for the ‘normal’ implantologist”
I will address points 2) and 3) in later posts – for this blog, I will focus on the idea that there are no long-term results from procedures with synthetic grafts as they lose their volume and resorb too quickly.
I hear this regularly and I understand why. Previous generations of synthetic materials were not perfect and did suffer from some of these problems. This was broadcast widely by some manufacturers of competitive, traditional materials. But it is simply not backed up by the science (and the personal experience of clinicians all over the world) surrounding modern alloplasts, in particular B-TCP.
Modern B-TCP (such as that used within EthOss) is a marvel of engineering. The porosity, particle size and particle stacking are all optimised to allow the material to resorb at the same rate as new host bone formation. The specific timeframes vary from patient-to-patient but usually, we see total material resorption and replacement by host bone within 24 months (often it is sooner).
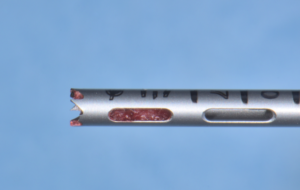
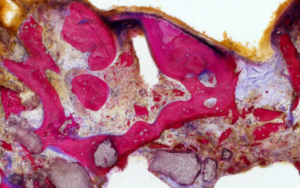
This is backed up by a significant body of research. The sample below is from one of my own studies with the histology and histomorphometry undertaken by the University of Freiburg. This core was taken from a patient prior to implant placement 12 weeks following a socket graft procedure. The second image shows the full sample with the last illustrating a close-up of a BTCP particle.
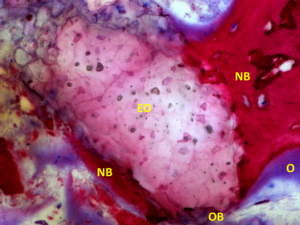
The close-up image is an ideal showcase of B-TCP at work. You can see the particle (EO) in intimate contact with the new bone (NB) with the presence of osteoblasts (OB) and osteoid formation (O). It’s a great way to see how the B-TCP is being broken down and resorbed. You can even see if you study closely that new bone growth is taking place throughout the B-TCP particle, not just around the edges (illustrated by the magenta-colouring throughout the EthOss particle). The full case study behind this sample can be viewed on the EthOss website here.
When the B-TCP has fully resorbed there will be no grafting material left in the site – just host bone. The idea that this bone will somehow lose all volume and resorb away after 4-5 years is strange. As long as the patient and the implant remain healthy it should continue to naturally remodel in line with Wolff’s law.
This is where modern alloplasts like EthOss are letting us move away from traditional “Guided Bone Regeneration” and towards “True Bone Regeneration”. We aren’t working with “filler” materials any more that will remain in the body long-term like xenografts or HA. We are working with regenerative materials that will upregulate the host healing response, putting the body back in the state it was in before the defect developed.
Long-term this means we are giving the patient the best possible outcome – their own bone, naturally turning over and remodelling, supporting their implant which should be fully integrated.
I have been using synthetic grafts exclusively in my practice for over 20 years and have performed over 6000 successful bone augmentation procedures. This has given me a massive library of cases to illustrate these points, but I’ve chosen just one to show here:
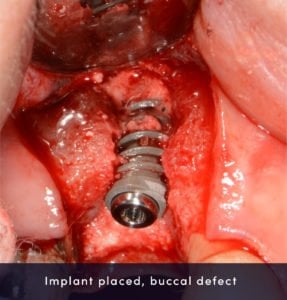


This case shows everything I’ve discussed above. You can see the initial defect, the graft placement and the long-term result.
This was an unusual case as the patient requested some soft tissue surgery 4 years later, and due to the frailness of the tissue I had to raise a flap to perform a Free Gingival Graft (rather than use a tunnel technique).
However, this does give us the opportunity to see the host regeneration long-term. This case is now loaded over 6 years without any problems. Without any complications I expect this implant to remain in function for a very long time, successfully supported by naturally remodelling host bone. You can view the full Case Study, including long-term scans, here.
I firmly believe this is the best outcome for any patient. It removes any ethical or religious concerns they may have about donor material and helps to maximise the chances of long-term success.